Inequalities: Rebalancing Act one year on
This week marks the first year since the launch of Rebalancing Act, a resource developed by Revolving Doors Agency, with support from Public Health England and the Home Office which looked at concrete ways in which partnership and collaboration can be strengthened to address the health inequalities faced by those in contact with the criminal justice system.
Revolving Doors Agency has been working for nearly 25 years to change systems and improve services for people who are caught in the revolving door of crisis and crime, as a result of their experience of multiple disadvantages, including mental ill health, substance misuse, domestic abuse and homelessness. Our independent research, policy and lived experience teams have been working together with government departments, local authorities and service providers across the public and voluntary sectors to develop and implement changes to address the social determinants, which over the life course, adversely affect health outcomes, offending behaviour and life chances.
Our research and our work with frontline practitioners, commissioners and people with lived experience have taught us that the relationship between health, social and economic equalities is complex; social exclusion can be both a cause and consequence of offending, and a cause and a consequence of poorer health. However, it is growing clear that the vast majority of people caught in the revolving door of crisis and crime have two distinct features in common: adverse childhood events and persistent poverty.
There is robust evidence that adverse childhood experiences (ACEs) can have a sustained, detrimental impact into adult life[1]. Individuals who experience ACEs can have lifetime effects, including dose-response relationships with multiple adverse outcomes, including poor physical and mental health and involvement in the criminal justice system. And these effects are large – people with four or more ACEs are 11 times more likely to be imprisoned or to use crack or heroin. A recent report found that if no individuals in the population were exposed to ACEs, the prevalence of incarceration amongst Welsh adults could be as much as 64.6% lower.
One adverse childhood event is the incarceration of a parent and here there is evidence that 65% of boys with a convicted parent go on to offend. The children of prisoners have at least double the risk of mental health problems compared to their peers, perhaps unsurprising as parental imprisonment can lead to stigma, bullying and teasing and, children of prisoners are often subject to unstable care arrangements, and face a negative financial impact on families, including financial instability, poverty and debt, and potential housing problems. Collectively, this constitutes substantially higher levels of social disadvantage than their peers.
It is encouraging to see, for example, Lancashire Constabulary beginning to explore how policing can respond to ACEs and, across the border, the Violence Reduction Unit’s public health approach to crime.
But if we are going to really address health inequalities of this population and address reoffending, we must also address the inequality that lie at the heart of each. Just this week we see that life expectancy has fallen since 2010 – the first in over 100 years – in the post-industrial and deprived coastal areas of England. These are exactly the areas found to have the largest populations of those with multiple needs, including criminal justice contact, substance misuse, homelessness and mental illness. Again we can see early evidence of dose-response relationships, between the number of austerity-related cuts and mortality. We need to respond to poverty as well as ACEs; they have unique but overlapping effects.
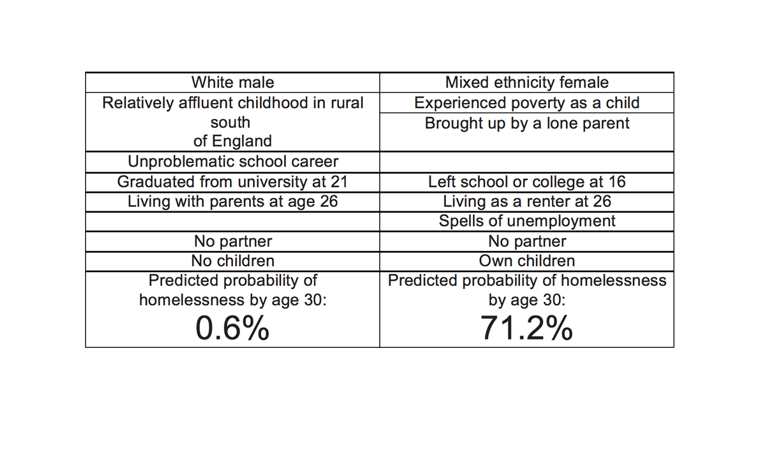
Of course, as Suzanne Fitzpatrick’s work below shows, poverty works in combination with other inequality.
I read recently about “glass floors”, the concept that there is a level of advantage that will prevent someone “falling through the cracks”. The family that takes someone back in, the hope of leaving an abusive home for university, the money to pay for substance misuse rehabilitation. And this concept seems to work for the stories we hear in our forums of people with lived experience: their stories often lack the advantages that would give a glass floor.
One year on from the Rebalancing Act, and in our 25th year, we are beginning to develop a new framework for action on prevention and early intervention. We continue to call for organisations to build the local partnerships – of Police and Crime Commissioners, public health, local authorities, the police and the NHS – that can really address the profound health inequalities of this vulnerable population. And we stand ready to help – just contact us. But we challenge each locality to build a response to both the impact of ACEs and the impact of inequality.
[1] The types of childhood trauma generally considered to form ACEs include physical abuse, sexual abuse, emotional abuse, physical neglect, emotional neglect, mothers treated violently, household substance misuse, household mental illness, parental separation or divorce and incarcerated household member.